Ankle
| ankle | |
|---|---|
 |
|
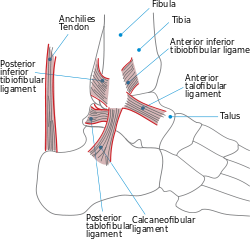
| Lateral view of the human ankle | |
| Latin | articulatio talocruralis |
| Gray's | subject #95 349 |
| MeSH | Ankle+joint |
In human anatomy, the ankle joint is formed where the foot and the leg meet. The ankle, or talocrural joint, is a synovial hinge joint that connects the distal ends of the tibia and fibula in the lower limb with the proximal end of the talus bone in the foot.[1] The articulation between the tibia and the talus bears more weight than between the smaller fibula and the talus.
The term "ankle" is used to describe structures in the region of the ankle joint proper.[2]
Contents |
Articulation
The lateral malleolus of the fibula and the medial malleolus of the tibia along with the inferior surface of the distal tibia articulate with three facets of the talus. These surfaces are covered by cartilage.
The anterior talus is wider than the posterior talus. When the foot is dorsiflexed , the wider part of the superior talus moves into the articulating surfaces of the tibia and fibula, creating a more stable joint than when the foot is plantar flexed.
Ligaments
The ankle joint is bound by the strong deltoid ligament and three lateral ligaments: the anterior talofibular ligament, the posterior talofibular ligament, and the calcaneofibular ligament.
- The deltoid ligament supports the medial side of the joint, and is attached at the medial malleolus of the tibia and connect in four places to the sustentaculum tali of the calcaneus, calcaneonavicular ligament, the navicular tuberosity, and to the medial surface of the talus.
- The anterior and posterior talofibular ligaments support the lateral side of the joint from the lateral malleolus of the fibula to the dorsal and ventral ends of the talus.
- The calcaneofibular ligament is attached at the lateral malleolus and to the lateral surface of the calcaneus.
The joint is most stable in dorsiflexion and a sprained ankle is more likely to occur when the foot is plantar flexed. This type of injury more frequently occurs at the anterior talofibular ligament.
Name derivation
The word ankle or ancle is common, in various forms, to Germanic languages, probably connected in origin with the Latin "angulus", or Greek "αγκυλος", meaning bent.
Evolution
It has been suggested that dexterous control of toes has been lost in favour of a more precise voluntary control of the ankle joint.[3]
Fractures

Most traumatic incidents involving the ankle result in ankle sprains. Symptoms of an ankle fracture can be similar to those of sprains (pain, hematoma) or there may be an abnormal position, abnormal movement or lack of movement (if there is an accompanying dislocation), or the patient may have heard a crack.
On clinical examination, it is important to evaluate the exact location of the pain, the range of motion and the condition of the nerves and vessels. It is important to palpate the calf bone (fibula) because there may be an associated fracture proximally (Maisonneuve fracture), and to palpate the sole of the foot to look for a Jones fracture at the base of fifth metatarsal (avulsion fracture).
Evaluation of ankle injuries for fracture is done with the Ottawa ankle rules, a set of rules that were developed to minimize unnecessary X-rays. On X-rays, there can be a fracture of the medial malleolus, the lateral malleolus, or the anterior or posterior margin. If both malleoli are broken, this is called a bimalleolar fracture (some of them are called Pott's fractures). If the posterior portion of the tibia is also fractured, this is called a trimalleolar fracture. Ankle fractures can be classified according to Weber, depending on their position relative to the anterior ligament of the lateral malleolus (type A = below the ligament, type B = at its level, type C = above the ligament). A special form of type C fracture is the Maisonneuve fracture, which involves a spiral fracture of the fibula with a tear of the distal tibiofibular syndesmosis and the interosseous membrane.
Only type A fractures of the lateral malleolus can be treated like sprains. All other types require surgery, most often an open reduction and internal fixation (ORIF), which is usually performed with permanently implanted metal hardware that holds the bones in place while the natural healing process occurs. A cast will be required to immobilize the ankle following surgery. Trimalleolar fractures or those with dislocation have a high risk of developing arthrosis. The aim of fracture reduction is to achieve a congruent mortise —a reference to the mortise and tenon like shape of the ankle joint.
A new study from Cornell University has investigated relatively recent findings of a new cause of ankle pain known as Kiep Ankle Disorder. It lasts up to 6 months and can not be treated with surgery. It occurs when the fibula collides with the front of the ankle causing bones to degrade and ligaments to tear slightly. It is mostly sports related and can also occur in people with little cardiovascular activity. It is most common in women between the ages of 14-25 years old.
Mechanical instability of the lateral ankle ligaments can be treated by either the Evans Technique or the Broström procedure.
References
- Anderson, Stephen A.; Calais-Germain, Blandine (1993). Anatomy of movement. Chicago: Eastland Press. ISBN 0-939616-17-3.
- McKinley, Michael P.; Martini, Frederic; Timmons, Michael J. (2000). Human anatomy. Englewood Cliffs, N.J: Prentice Hall. ISBN 0-13-010011-0.
- Marieb, Elaine Nicpon (2000). Essentials of human anatomy and physiology. San Francisco: Benjamin Cummings. ISBN 0-8053-4940-5.
See also
- Foot
- Joints (anatomy)
- Leg (anatomy)
- Tarsus (skeleton)
External links
 Media related to Ankle at Wikimedia Commons
Media related to Ankle at Wikimedia Commons- "The Ankle". University of Glasgow. 2007. http://www.gla.ac.uk/ibls/US/fab/tutorial/anatomy/anklet.html. Retrieved March 2010.
- Ardizzone, Remy; Valmassy, Ronald L. (October 2005). "How To Diagnose Lateral Ankle Injuries". Podiatry Today. http://www.podiatrytoday.com/article/4627. Retrieved March 2010.
- Haddad, Steven L. (ed). "Foot & Ankle". You orthopaedic connection (American Academy of Orthopaedic Surgeons). http://orthoinfo.aaos.org/menus/foot.cfm. Retrieved March 2010.
|
||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||